
Health inequalities and mitigating risks of digital exclusion
A guide for policy makers, providers and commissioners from a voluntary and community sector perspective
Mainstreaming the use of digital channels, products and services in health and healthcare has accelerated since the start of the pandemic. Although the Public Sector Equality Duty (Equality Act 2010) and other legislation do not explicitly require consideration of digital access and related barriers, it is clear that the move towards digital services may impact on inequalities for patients and service users regarding their ability to access health services and the outcomes achieved for them.
In November 2021, the independent report by Laura Wade-Gery identified that the challenge, as we emerge from the pandemic, is to capitalise on existing momentum by ‘Putting data, digital and tech at the heart of transforming the NHS’ while simultaneously ‘getting the basics right’. The first three recommendations in the review situate digital inclusion and digital transformation within the wider context of health inequalities, and point to the core principles of being person-centred and aiming for a fully inclusive NHS:
- Recommendation 1: Commit to a patient and citizen centred organising principle for future service transformation
- Recommendation 2: Consider and mitigate digital inequality in all service transformation. Expand the role of the SRO for Health Inequalities to include digital inequality
- Recommendation 3: Commit to building patient and citizen trust and acceptance in the use of health data to improve outcomes. Provide more efficient access to data for analytics that ensures privacy and can be used to improve care delivery.
The importance and scale of change – cultural as well as technological – required to achieve this shift are foregrounded. The review recognises both the ways in which digital approaches can improve access, and also exclude people with low digital access or skills. As Wade-Gery states:
‘It will take focus to ensure the push for digital ways of working can help tackle these health inequalities rather than exacerbate them. NHSEI should develop national frameworks, guidance and best practice in designing and implementing digital solutions to reduce inequalities. When designing new models of care, these should include a choice for citizens between remote and face-to-face care. It is important this issue is managed actively. As such, the responsibility of the NHSEI Health Inequalities team should be expanded so that digital exclusion is seen as another lens within health inequalities.’
In response, mitigating against digital exclusion risks is one of five priorities that NHS England has set for system action to reduce health inequalities. The new Digital Health and Social Care Plan (2022) identifies digital inclusion as an issue (as well as user centred design and workforce digital skills), and commits to producing a framework by May 2023 for NHS action on digital inclusion as part of future plans, and further resources to support systems in practical action.
Digital exclusion is complex and complicated. While terms like ‘the digital divide’ are valuable for raising awareness and highlighting inequalities, the realities of digital exclusion are better understood as a spectrum – where digital access (devices, data connectivity), accessibility, skills, confidence, motivation and availability of support all combine to shape how people use the internet, and the balance of benefits and harms they derive from the digital world.
Research underway (led by the University of Liverpool) to set a benchmark for UK households – a ‘Minimum Digital Living Standard’ – has developed the following definition:
‘A minimum digital standard of living includes, but is more than, having accessible internet, adequate equipment, and appropriate training and support. It is about being able to communicate, connect and engage with opportunities safely and with confidence.’
Ensuring people achieve a minimum digital standard of living is not the responsibility of the NHS but – alongside government, industry, civil society and communities – the NHS, Integrated Care Boards and Partnerships, Primary Care Networks, GPs and others all have a part to play in digital inclusion. Identifying and implementing this will be essential for an inclusive recovery for all. Assessing progress is challenging as data on the causal links between health inequalities and digital inequalities is under-developed, though the scale of digital exclusion is clear:
- 1.5 million UK households don’t have internet access (Ofcom Adults’ Media Use 2022)
- 2 million households struggle to afford broadband or mobile data (Ofcom Affordability 2022)
- 10 million adults lack even the most basic digital skills (UK Essential Digital Skills 2021)
- 14.9 million adults have low or very low digital engagement (Consumer Digital Index 2021)
As Wade-Gery advocates: ‘Now is the moment to put data, digital and technology at the heart of how we transform health services … Greater focus at the centre on the needs and experience of diverse users, including addressing inequalities, would facilitate transformation.’
We hope this guide supports such a focus.
This short guide aims to help policy makers, commissioners and service providers working in different parts of the health system in England – including those working in:
- NHS England
- Integrated Care Systems and Integrated Care Boards
- Other members of Integrated Care Partnerships – including local authorities, voluntary and community sector organisations
- Primary Care Networks, General Practice and other local health care providers.
We hope this guide will be used to:
- Stimulate and support discussions about inclusive approaches to using digital channels, products and services in primary and secondary care;
- Consider how digital exclusion intersects with protected characteristics and health inequalities;
- Consider what mitigations can help to reduce digital exclusion risks;
- Save people time by curating relevant resources and existing toolkits;
- Support a greater focus at the centre on the needs and experience of diverse users of health care services, addressing digital and health inequalities.
This guide does not provide all the answers, but it does provide an overview of factors to consider and suggestions for how to mitigate digital exclusion risks.
This guide has been developed by Good Things Foundation, in our role as a member of the VCSE Health and Wellbeing Alliance.
The guide is not based on a systematic evidence review; it draws on our knowledge of existing evidence and our experience as a digital inclusion charity (including from delivering the NHS England / NHS Digital Widening Digital Participation programme between 2013 and 2020). We have supplemented our knowledge with input and insights from voluntary and community sector organisations through the VCSE Health and Wellbeing Alliance and our national digital inclusion network of community partners. In line with this approach, a list of useful resources (including research reviews and toolkits) is provided at the end, rather than referencing throughout.
Where we identify potential evidence gaps, these may reflect gaps in our awareness rather than in the evidence base. Overall, there is apparently less – and less robust – evidence on solutions than on barriers. Research funders such as the National Institute for Health Research are working to address this. Therefore, suggested mitigations and solutions in this guide are largely drawn from the evidence, insights and experience of voluntary and community sector organisations.
Our starting point was to consider digital access barriers and solutions with regard to different protected characteristics, inclusion health groups, and people who may face higher risk of worse health access and patient outcomes due to wider socio-economic factors. Intersectionality (how inequalities based on forms of discrimination and disadvantage ‘intersect’) shapes the experience of many people within these groups.
Section 2 sets out common digital access barriers – relevant across different groups. Section 3 sets out potential mitigations or solutions – starting with some general pointers; followed by a summary of solutions segmented by relevance to people working at (a) system or strategic level; (b) service or local delivery level; (c) commissioning digital services or tools; (d) designing digital services or tools. A final table in this section maps potential mitigations against barriers (split by design and delivery). Section 4 summarises additional considerations related to protected characteristics, inclusion health groups, and other groups at risk of being under-served or worse health outcomes. Section 5 is a list of references and useful resources.
Section 2: Common barriers across groups
2.1 Introduction
This section sets out some common, cross-cutting barriers which are relevant across all protected characteristics and inclusion health / health inequalities groups. These are:
- Access (e.g. device, data connectivity)
- Skills and confidence
- Motivation
- Trust
- Space (physical)
- Support (social or specialist)
- Independence, choice and control.
The briefing paper, ‘Digital exclusion and health inequalities’ (Good Things Foundation 2021), is a useful overview; also ‘Digital technology and health inequalities: A scoping review’ (Public Health Wales 2020) and ‘Unlocking the digital front door: keys to inclusive health care’ (National Voices 2021). Additional resources and research are listed in Section 5.
2.2 Digital barriers – areas to consider across different groups and characteristics
- Internet access – there are many aspects which all have to be in place (alongside having the skills and/or support to use the internet safely and confidently):
- Good mobile or broadband coverage, speed and signal
- Suitable, appropriate device to access a digital service (via app / browser)
- Sufficient data to access the digital service
- Sufficient electricity to keep their device charged
- A printer or easy access to a printer (may be required or assumed)
- Choice: not using the internet is a personal, positive choice for some; for others,it reflects other factors (e.g. fear, anxiety, cost, mistrust, lack of support – including from family)
- Basic digital skills for life (see Essential Digital Skills for Life, Gov.uk)
- For example: has an email or social media account; can find and download an app; use a search engine; understand ‘padlock’ sign; avoid online fraud, scams, etc; use video calling; use online forms (e.g. for appointments)
- No, low and limited digital literacy can overlap with other areas of skills:
- Basic literacy and numeracy
- English (or Welsh) language proficiency
- Health literacy – e.g. understanding patient information, knowing where to find trustworthy information and help such as NHS 111
- Media literacy – e.g. understanding not everything on the internet is true
- Confidence to apply digital skills in practice and use the internet for health or care
- Low motivation to use a digital service or tool; this might reflect:
- Concerns about digital services replacing face-to-face or phone in general
- Concerns about losing the option to access / revert to face-to-face support
- Lack of confidence to use a digital service, and use it safely and independently (e.g. in case you don’t have access to support when needed)
- Lack of belief that the digital service will deliver a better or faster outcome
- Lack of support – impacting on confidence and belief in the value of digital
- Low trust or mistrust of the NHS / GP / other health or care providers
- Concerns about who (e.g. in a GP or hospital) has access to data (e.g. who might see an image sent to a GP to support a remote consultation)
- Concerns about digital services replacing face-to-face or phone services
- Low trust arising from non-digital past experiences (heightened where low health literacy, low understanding of how health systems work, reliance on translators)
- Low trust or mistrust of technology generally
- Concerns about surveillance technology, cybersecurity risks
- Concerns about how personal data will be used, shared and kept safe
- Concerns about technology going wrong
- Concerns about misinformation and disinformation, fraud and scams
- Low trust in one’s own abilities to use technology, especially where access to tech support is limited and/or would have to be paid for.
- Access to a private and/or safe and confidential space to use the internet
- For example, to do an online health consultation or for remote monitoring, or anything where confidentiality, privacy and security are required
- Factors impacting negatively on this include:
- Not having a personal device with sufficient mobile data
- Reliance on using a shared device kept in a public or common area
- Living in overcrowded housing or housing with limited private space
- Living in an abusive home environment
- Temporary or transient accommodation (impacts on data connectivity)
- Evidence suggests a positive relationship between internet use and confidence and people’s personal social relationships (having a social network)
- Living alone in older age and for disabled people is an additional risk factor for not using the internet at all, or only using it for very few things
- Evidence shows the value of being able to access in-person, local and friendly support to use the internet and develop digital skills and confidence over time
- For example, in community centres, lunch clubs, carers groups, homelessness hostels, libraries, care homes, and (where offered) in hospitals, GP and other health or care settings
- Awareness is low about available support
- To build digital skills and confidence (e.g. Good Things Foundation, LearnMyWay)
- To improve accessibility for disabled people (e.g. AbilityNet’s helpline; free software to support accessibility)
- To train practitioners to be digital champions (e.g. Digital Unite’s training).
- As long as people have the tools, skills and support in place – then digital health and care technology can have positive impacts on both access and outcomes:
- Enabling greater independence by reducing reliance on others
- Enabling better use of people’s time and money by reducing unnecessary travel and allowing people to access services at times that suit them
- Supporting self-care – for example through remote monitoring devices
- Not everyone will want to, or be able to, use digital health and care tools safely
- Keeping all channels open is essential to avoid discriminating against people who lack the access, skills, trust and support to use digital services
- Everyone can experience times of greater ‘vulnerability’ to online harms (for example, at times of stress or life transition)
- Evidence shows growing use of ‘proxies’ to access digital services and do online transactions (e.g. family, friends, carers acting on someone’s behalf); this carries
- Implications for data privacy and security
- Implications for choice and control, and decision-making and consent
Section 3: Potential mitigations or solutions
3.1 Introduction
This section focuses on potential solutions or mitigations to digital exclusion barriers which different actors could influence, including NHS system partners, Integrated Care System Boards and Partnerships, Primary Care Networks, GPs and other healthcare providers. Some solutions require coordination and collaboration from other sectors and providers.
It is important to note that there is less evidence on solutions than barriers. The suggestions below are drawn from available evidence and the insights and experience of voluntary and community sector organisations working with groups facing health inequalities and digital barriers.
Useful resources with a solutions focus are: ‘Inclusion Health Audit Toolkit’ (Inclusion Health 2020); ‘Digital inclusion in health and care: Lessons learned from NHS Widening Digital Participation’ (Good Things Foundation 2020); ‘Involving people and communities in digital services’ (NHS); ‘Digital inclusion in mental health toolkit’ (NHS Confederation 2020), and ‘Inclusive Digital Transformation’ (Thrive by Design 2022). There is also the Accessible Information Standard and the Digital Technology Assessment Criteria. More research and development is underway funded by NHS, public, commercial and charitable bodies.
For those working in the NHS in England, internal tools available to support programmes include the FutureNHS Equalities and Health Inequalities Network site, and the Health Inequalities Improvement Planning Matrix for NHSEI programmes/workstreams. NHS England’s Health Inequalities Improvement team will play a key role in collating and curating resources on mitigating digital exclusion risks as part of the approach to reducing health inequalities.
3.2 Potential mitigations or solutions: general points
- Patient choice and equitable access are key NHS principles. Keeping non-digital means of accessing a quality health service or information is vital to avoid discriminating against those who cannot (or choose not to) use digital health or care services – alongside making digital services as inclusive as possible – in design and delivery
- Digital technology can help to remove barriers to accessing health services which have been experienced by poorly served groups, where digital access and support is in place. Barriers to accessing digital services can also reflect and compound non-digital barriers.
- Some steps to mitigating digital exclusion risks will not be appropriate or adequate for all:
- For example, asking if someone has a private space to use a remote service may not be sufficient mitigation if someone is in a domestic abuse situation
- Having a family member who can support use of digital services can be helpful but may not be appropriate – especially where children are asked to provide help
- Digital goalposts are constantly shifting on all sides:
- People’s use of digital services can go up or down for different reasons
- Patient-facing interfaces with digital services change as improvements are introduced; this can be confusing for patients and healthcare professionals
- A growing marketplace for health-related technology means a variety of layouts, interfaces, functionalities; this lack of standardisation creates challenges for people with low digital skills and confidence, and those who support them
- Co-production with patient users, and also with practitioners and trusted intermediaries (e.g. VCSE partners) can improve service design and needs to include people across age groups and from marginalised groups – including people with lower digital skills.
- Strategies to improve digital inclusion (whether among a patient cohort, an under-served group, in a locality or across an Integrated Care System) should:
- Take a holistic view of digital inclusion – reflecting that digital access, skills and confidence are relevant across people’s lives – a wider determinant of health
- Include, but not focus narrowly on, providing support with digital health literacy and accessing NHS and GP services and pathways digitally
- Involve and commission digital inclusion services from voluntary and community sector organisations with reach, trusted relationships and experience to support.
- Some potential solutions raise questions about resources, roles and responsibilities. For example, what is in scope for different healthcare professionals, or for VCSE partners?
- Achieving digital inclusion for the population is not the sole responsibility of the NHS or healthcare providers – but the NHS, Integrated Care Boards and Partnerships, Primary Care Networks, GPs and others have a key part to play.
3.3 Overview of potential mitigations or solutions by role or remit
This section summarises the range of mitigations or solutions that could be considered, segmented by relevance to people working at:
- System level or in strategic commissioning roles
- Service level – in implementation or delivery roles
- Service level – in service design or user research roles
- System or service level – in workforce development and management roles.
We’ve organised the material in this way to support use by different audiences – recognising differences in roles and remits. We’d encourage everyone to look at all sections, however, as none of these sit in isolation from each other. (For information: in the next section (3.4), potential mitigations or solutions are mapped against the specific barriers identified in Section 2 – e.g. access, skills, trust).
- Keep open ‘traditional’ (non-digital) means of accessing a quality health/care service.
- These should be easy to find to avoid discriminating against people who cannot or choose not to use digital services
- Commission for ‘inclusive by design’ – to enable more people to use a digital service independently.
- Map local provision of settings which help people to access digital services, and understand local needs for support
- Use this to inform strategic commissioning and fund or part-fund digital inclusion as part of an inclusive digital transformation strategy
- Identify settings offering a safe, confidential space to access digital services
- Identify settings offering help to access free devices and data
- Encourage provision of free, easy to use access to secure WiFi in health and social care settings – such as GP surgeries.
- Encourage expansion or setting up of digital inclusion hubs in communities so people know where to get help to use the internet – including (but not limited to) accessing health services and information safely
- Use existing community assets where possible
- Commission or find appropriate ways to provide funding for voluntary and community sector organisations who are best placed to support digital inclusion
- Ensure clear referral routes between health system partners and voluntary and community sector providers of digital inclusion support
- Seek to reduce ‘data poverty’ barriers through securing ‘zero-rating’ (i.e. no data connectivity charges to the patient) for NHS / health digital services
- Where available, promote these sites widely
- Promote and ensure explicit consideration of digital access barriers (and how these intersect with protected characteristics and other drivers of health inequalities) when undertaking Equalities and Health Inequalities Impact Assessments for design and implementation of patient-facing digital services for health, or use of digital in pathways
- Promote use of social prescribing to help people who are digitally excluded to:
- Access a free device and data connectivity to support them
- Get help to build digital skills and confidence generally, as well as to access health and wellbeing support specifically
- Promote the benefits of using digital for health to motivate uptake among people with access and skills, alongside reassurance about maintaining non-digital channels
- Contribute to building the evidence base – through evaluations, research and systematic analysis of feedback from patients, carers and practitioners for continuous improvement
- Wherever possible, provide spaces within GP surgeries or other health care settings so patients or carers can access digital health and care services, ideally with:
- Support (e.g. from a digital champion)
- Access to a device in the setting, and free public WiFi for those with their own
- An appropriate level of privacy
- Ask patients about their ability to use the internet as part of a health or care record (rather than make assumptions) – including personal access and ability to use the internet in private
- Ask patients if they:
- Know someone they trust who can help them use a service (if appropriate)
- Already use assistive technologies
- Have accessibility needs which digital could address
- Ask health or care practitioners to check if a patient or service user can use the digital service in a private, safe and confidential space. Note: This will not be adequate mitigation if someone is in a domestic abuse situation
- Reassure that a real person will be there in case things go wrong, and people can still get ‘in person’ support
- Be aware that negative experiences of filling in official forms (including paper) can impact negatively on motivation and confidence in using digital services
- Consider facilitating peer support (e.g. via WhatsApp) among those using it
- Consider using social prescribing to help people who are digitally excluded to:
- Access a free device and data connectivity to support them
- Get help to build digital skills and confidence in general (as well as to access health services and information online)
- Use simple ways to get feedback from patients or carers using a digital tool or pathway
- Ideally ask a question to map feedback against people’s digital confidence
- Equip health/care workforce with knowledge so they can answer questions from patients about:
- the benefits and value of using the specific digital service
- how people’s data will be used, stored and shared
- where to get help and who to contact if things go wrong
- Train digital champions who can help (ideally in the same language where people have limited English skills):
- Guide people to register for and use a digital service
- Help people improve the accessibility of their devices
- Take a broader (non-medical) view of digital inclusion
- Advise on where to get help with digital access and skills
- Equip social prescribing link workers to
- Support digital inclusion in the local community in general, as well as for accessing health services – taking a broader (non-medical) view
- Develop links with voluntary and community sector organisations with experience of providing digital inclusion support – and commissioned to provide this support
- Aim for ‘inclusive by design’ standards to enable more people to use a digital service independently. This will also make it easier to show people how to use it. As part of this:
- Take all literacy or skills into account, not only digital literacy – also health literacy, media literacy, basic literacy and numeracy, English language skills
- Take ‘data poverty’ into account – designing websites and tools which do not consume high levels of mobile or broadband data, or require fast speeds
- Conduct user research and testing with people who have limited data connectivity and low digital skills (part of testing with marginalised groups)
- Involve ‘trusted intermediaries’ in design – these are people in health, care, community and voluntary sectors who may be asked by patients for help in using the digital service
- Identify practical ways digital access can reduce existing barriers for poorly served groups or inclusion health groups; design to make this happen
- Use familiar platforms – where people are online already and feel comfortable
- Use WhatsApp / messaging to support better communication
- Provide clear, plain language information on:
- How personal data will be used and kept safe
- Who will have access and whether data will be shared (e.g. Government departments)
- Use design features that make it easier for people – consider features such as:
- Low data usage (option/default)
- Translation into other languages
- Sub-captions and audio
- Low data usage as an option
- Ability to tailor, adjust settings or use with accessibility tools
- Useability and accessibility
- Easy to find (especially if it may not be used daily)
- Easy to register (verify identity)
- Easy to open up (passwords, verification and authentication)
- Easy to use and navigate
- Easy to understand
- Relatable and personalisable (designed ‘for people like me’)
- Easy to integrate into daily life
- Motivation to use a digital service may be higher where:
- Transactional (e.g. booking an appointment) rather than relational (e.g. a consultation)
- Convenience is a ‘quick win’ – saves time, money, flexible
- Good reviews – use is endorsed and encouraged by others
- Supports better communication between patient and provider
- Trust in a service may be higher if:
- Technically it works – no error pages, easy to navigate
- Jargon-free simple language
- Reassurance that a real person will be there if things go wrong
- Reassurance that a real person will receive the information, followed by communication to the patient on what will happen
- Reassurance that personal data will not be shared with third parties without permission
- Good reviews – use is endorsed and encouraged by others
- Create options for people to get help when they’re using an online service:
- Accessible, printable guides
- Easy to find information on how to get help by phone
- Easy access to a ‘real person’
- Use simple ways to get feedback; ideally ask a question to map feedback against people’s digital confidence
3.4 Potential mitigations to specific barriers
This section presents the potential mitigations or solutions (summarised in the previous section) – this time mapping solutions against the specific barriers identified in Section 2:
- Digital access
- Digital skills and confidence
- Motivation
- Trust
- Space (physical) – not having access to suitable space
- Support (social, specialist) – not having access to appropriate support.
For each barrier identified, the potential mitigations are divided by relevance to ‘design’ or ‘delivery’ of patient-facing pathways, products and services which use digital technologies.
Design solutions
- Conduct user research and testing with people who have limited data connectivity (as part of user testing with marginalised groups generally)
- Design digital health/care services with a ‘low data usage’ option (or default)
- Keep open ‘traditional’ (non-digital) means of accessing a quality health/care service. This should be easy to find to avoid discriminating against people who cannot or choose not to use digital services
- Identify practical ways digital access can reduce existing barriers for poorly served or inclusion health groups; design the service to make this happen
- Use familiar platforms – where people are online already and feel comfortable
Delivery solutions
- Provide free, easy to use access to secure WiFi in health and social care settings (and access to devices and support). Consider using the community based ‘digital health hubs’ model
- Secure ‘zero-rating’ (no data charges to user) for NHS, GP & care services
- Promote ‘zero-rated’ NHS sites widely – including primary care networks, VCSE partners
- Use social prescribing to help people who are digitally excluded to:
- Access a free device and data connectivity to support them
- Get help to build digital skills
- Ask patients about their ability to use the internet as part of a health or care record (rather than make assumptions)
Design solutions
- User research and testing with people who have low or limited digital skills and confidence (as part of testing with marginalised groups more generally)
Go beyond the government Website Accessibility Guidelines and take all literacy or skills into account:- Digital literacy, health literacy, media literacy (e.g. fake news, scams), basic literacy and numeracy, English language
- Consider design features to support:
- Translation into other languages
- Sub-captions and audio
- Low data usage as an option
- Ability to tailor, adjust settings or use with accessibility tools
- Useability and accessibility
- Create options for people to get help when they’re using an online service (continuous improvement is a strength but can create confusion for users):
- Accessible, printable guides
- Easy to find information on how to get help by phone
- Access to a ‘real person’ to help
- Use simple ways to get feedback; ideally ask a question to map feedback against people’s self-reported digital confidence
- Use familiar platforms – where people are online already and feel comfortable
- Use WhatsApp / messaging to support better communication
Delivery solutions
- Ask patients about their ability to use the internet (access, skills and confidence) as part of a health or care record (rather than make assumptions)
- Ask patients if they:
- Know someone they trust who can help them use a service
- Already use assistive technologies
- Have accessibility needs which digital could address
- Train digital champions who can help (in the same language where possible):
- Guide people to register for and use a digital service
- Help people improve the accessibility of their devices
- Take a broader (non-medical) view of digital inclusion
- Advise on where to get help with digital access and skills
- Advise on what NHS sites to use, how to avoid ‘NHS’ scams or health mis/disinformation
- Use social prescribing to help people who are digitally excluded to:
- Access a free device and data
- Get help to build digital skills
- Expand or set up community ‘digital health hubs’ so people know where to get help to use digital health services
- Funding for VCSE partners
- Ensure clear referral routes
- Review strategic commissioning roles of health/care system leaders to fund or part-fund digital inclusion
Design solutions
Consider features to increase motivation to use a service, and keep on using it:
- Easy to find (especially if it may not be used daily or regularly)
- Easy to register (identity verification)
- Easy to open up (passwords, verification and authentication)
- Easy to use and navigate
- Easy to understand (complies with Accessible Information Standards)
- Relatable and personalisable (feels designed ‘for people like me’)
- Easy to integrate into everyday life
Motivation to use a digital service (and keep using it) may be higher where:
- The purpose is transactional (e.g. booking or confirming an appointment, ordering a prescription) rather than relational (e.g. a consultation)
- Convenience is a ‘quick win’ – saves time, money, flexible around life
- Good reviews – use is endorsed and encouraged by other people – peers, family, friends, health professionals
- Reassurance that a real person will ‘be there in case things go wrong’
- Supports better communication between patient and provider
Delivery solutions
- Promote the benefits of using digital health services – along with information about where to find out more (locally and online)
- Equip health/care workforce with knowledge so they can answer questions from patients about:
- the benefits and value of using the specific digital service
- Train digital champions who can help:
- Guide people to register for and use a digital service
- Help people improve the accessibility of their devices
- Reassure that a real person will be there in case things go wrong, and people can still get ‘in person’ support
- Consider facilitating peer support (e.g. via WhatsApp) among those using it
- Expand or set up community digital inclusion hubs, so people know where to get help to use digital health services – using existing community assets
- Find appropriate ways to fund voluntary and community sector organisations
- Ensure clear referral routes – building bridges between healthcare providers and voluntary and community sectors.
Design solutions
As part of compliance with Accessible Information Standards, Patient Information Standards, and GDPR legislation:
- Give clear, plain language information:
- How personal data will be used
- How data will be kept safe
- Who will have access and whether data will be shared (e.g. Government departments)
- Trust in a service may be higher if:
- Technically it works – no error pages, easy to navigate
- Jargon-free simple language
- Reassurance that a real person will be there if things go wrong
- Reassurance that a real person will receive the information, followed by communication to the patient on what will happen next, and when
- Reassurance that personal data will not be shared with third parties without permission
- Good reviews – use is endorsed and encouraged by others
Delivery solutions
- Equip health/care workforce with knowledge so they can answer questions from patients about:
- how people’s data will be used, stored and shared
- the benefits and value of using the specific digital service
- who to contact if things go wrong when using a service
- When supporting people, be aware that anxieties and past negative experiences of using paper-based processes or filling in official forms can lower motivation, trust and confidence in using digital services
- Expand or set up community ‘digital health hubs’ so people know where to get help to use digital health services
- Funding for VCSE partners
- Ensure clear referral routes
Design solutions
- As part of a health or care record – consider asking about personal internet access, skills and confidence, including ability to use the internet in private to access health or mental health support
- This would need updating as internet use goes up and down
- Some people may not disclose or feel able to answer this
Delivery solutions
- Ask health or care practitioners to check if a patient or service user can use the digital service in a private, safe and confidential space. Note: This will not be adequate mitigation if someone is in a domestic abuse situation
- Encourage GP surgeries to have spaces where people can access digital health and care services, ideally with support, devices and WiFi, and some privacy
- Map local provision of health, care and community settings which offer a safe, confidential space to access services
Design solutions
- Aim for ‘inclusive by design’ to enable more people to use a digital service independently. This will also make it easier to show people how to use it.
- Features like chatbots or chatting online with a person to navigate a service are good; but more likely to be used by people with higher digital skills
- Easy access to ‘real person’ support needs to be available (e.g. by phone)
- Involve ‘trusted intermediaries’ in design – these are people in health, care, community and voluntary sectors who may be asked by patients or service users for help in using the digital service (as well as involving patients and health/care professionals)
- Think about design features which help the service feel personal and caring – rather than impersonal, and support better communication between patients and providers.
Delivery solutions
- Provide free, easy to use access to secure WiFi in health and social care settings – such as GP surgeries – plus access to devices and support; consider the ‘digital health hubs’ model
- Ask patients about their ability to use the internet as part of a health or care record (rather than make assumptions)
- Ask patients if they:
- Know someone they trust who can help them use a service
- Already use assistive technologies
- Have accessibility needs which digital could address
- Be aware that negative experiences of filling in official forms (including paper) can impact negatively on motivation and confidence in using digital services
- Use WhatsApp / messaging to support better communication or peer support
- Equip health/care workforce with knowledge so they can answer questions from patients on the service
- Train digital champions who can help (in the same language where people have limited English language skills):
- Guide people to register for and use a digital service
- Help people improve the accessibility of their devices
- Take a broader (non-medical) view of digital inclusion
- Advise on where to get help with digital access and skills
- Advise on what NHS sites to use, how to avoid ‘NHS’ scams or health mis/disinformation
- Use social prescribing to help people who are digitally excluded to:
- Access a free device and data connectivity to support them
- Get help to build digital skills
- Expand or set up community ‘digital health hubs’ so people know where to get help to use digital health services
- Fund VCSE partners
- Ensure clear referral routes
- Map local provision of settings which help people to access digital services, and understand local needs for support
Section 4: Specific groups – additional and priority areas
4.1 Protected characteristics
This section identifies specific or additional areas relevant to protected characteristics. The main protected characteristics impacted by digital exclusion are age (especially older age) and disability. These often intersect with other characteristics (e.g. digital exclusion compounds significant health inequalities faced by Gypsy, Roma and Traveller communities). There is little evidence on digital access and some protected characteristics (e.g. religion and belief). Pregnancy and maternity is an area of growing interest, given the growing use of digital for pregnancy and maternity support.
- Older people, aged above 65 years old, and especially above 75 years old, are significantly more likely to be non-users or lapsed users or limited users of the internet.
- Older age remains the most significant predictor of non-use of internet
- This is more marked for older people on low incomes and living alone
- The highest proportion of non-users of the internet is in the cohort of 75+ years
- Around 500,000 people (predominantly 75+ years old) stop using the internet each year, often related to health conditions and impairments
- Older people are more likely to express:
- Lack of interest in using digital services or apps (‘not for people like me’)
- Fears around security, complexity, technology breaking, and not being confident to use digital services independently
- Preference for in-person or phone support (also links to loneliness and isolation)
- Assumptions should not be made about digital access and internet use due to age; this is particularly relevant for older age groups but also relevant for younger age groups.
- Low digital access and skills primarily reflect factors other than age (although there is still an age gradient), especially low income and low educational attainment.
- Consider digitalisation of services relating to parenting roles: Parents with lower digital access and skills may struggle to use digital services and not experience potential benefits (e.g. convenience, reducing travel, saving money, and accessing support around work and caring)
- Extended working lives, remote working and use of digital in the workplace means that having basic digital skills for work, as well as life, has become more important; not having these skills is a more likely for people in mid-life and later life (e.g. 50+ years old)
- Generally high levels but levels of personal access and ability to use the internet for more than a few things (e.g. gaming or social media) can vary widely (factors: looked after or care leaver status, household income, education, housing situation)
- Some evidence that warns against making assumptions about young people’s preferences for digital services over face-to-face or in-person support
- Digital 24/7 access is important but with options to see someone in person
- Reassurances about privacy and confidentiality can be especially important
- Exposure to online harms and media literacy is a key issue (e.g. critical understanding of health information and whether it is from a trustworthy source)
- Digital (and assistive technology) can bring major benefits to health, wellbeing, independence, choice and control for disabled people
- Low digital access and use correlate with age, income and educational level
- Compliance with Accessible Information Standards and Website Accessibility Guidance still varies and impacts on people’s user experience and outcomes
- Use is also negatively impacted by not having one or more of the following:
- Suitable size and type of device to meet impairment-related needs
- Skills &/or support to adjust accessibility settings on the device
- Skills &/or support to get additional accessibility software or kit to make using the internet easier, including ease of finding what you need
- Sufficient data to support potentially higher levels of data usage related to disability (e.g. for using additional software, taking more time to use)
- Anxieties, accessibility barriers, past negative experiences of using paper-based processes to access official (NHS, government) support can impact negatively on people’s motivation, trust and confidence in using digital services
- Assistive technology – awareness and use is lower among older age groups.
- Digital and assistive technology can bring major benefits for independence, choice and control for people with mental health conditions and long-term conditions, where people have the required level of access, skills and support (see above):
- Self-care and self-management of conditions
- Access to online and blended peer support as well as professional support
- Convenience and flexibility to suit the individual
- Saving time and money where reduced need to travel for appointments
- Potential for a more person-centred experience (depending on design)
- Internet use can worsen mental health conditions through exposure and increased vulnerabilities to online harms (e.g. sites encouraging suicide)
- Lack of evidence of specific digital barriers. Some evidence of higher risks of exposure to online harms (online abuse, hate speech, harassment) with harmful effects on physical and mental health. This may have additional impacts on confidence, motivation and trust
- Lack of evidence found on specific digital barriers
- Limited but growing evidence about the digitalisation of pregnancy and maternity services and potential implications for inequalities
- Intersectionality with other protected characteristics (e.g. age, disability, race and ethnicity – Gypsy, Roma and Traveller communities; refugees, people seeking asylum and migrant communities, sexual orientation)
- Intersectionality with inclusion health groups (e.g. living on a low income).
- During lockdown
- Digital support was found to have an important role to play but online and phone-based service delivery had limitations; face-to-face relational support needed for pregnant women, birthing people, babies and younger children.
- Online health information (e.g. NHS-approved Baby Buddy App) valued but with some risks of feeling anxious or overwhelmed by so much information.
- In domestic abuse situations, it isn’t sufficient to ask people if they have access to a private space to access support digitally.
- Also relevant: digitalisation of services for parents and children in early years, especially first-time parents. For example, planned roll-out of the eRed Book from April 2023
- Evidence of ethnic inequalities in digital access to services, but these are not uniform across services, settings or groups.
- Evidence in some studies of ethnic minority groups using health apps less often, or expressing lower trust or more concern about how their personal data will be used.
- For Bangladeshi people, particularly for those living in deprived areas, evidence of ethnic inequality in referral to urgent and emergency care services by NHS Direct. More generally, evidence of lower use of NHS Direct phone services by most ethnic minority groups compared to the White British group.
- Lack of sufficiently robust evidence on differences by ethnicity in digital access and use reflecting sample sizes which are too small. Differences appear minimal in national data, reflecting the younger age profile of many ethnic minority groups; but experience in communities points to strong intersectionality with characteristics such as older age and living on a low income.
- Gypsy, Roma and Traveller communities experience the worst health outcomes, and face barriers around digital access and skills – overlapping with low literacy
- Refugees, people seeking asylum, migrants may face:
- Identity verification barriers to registering for online NHS and GP services
- English language barriers (potentially alongside other literacy barriers)
- Low understanding about how the healthcare and social care system works
- Differences in entitlements to health and care support by citizenship status
- Refugees, people seeking asylum, migrants, Gypsy, Roma and Traveller communities can also have low trust and mistrust in digital public services:
- Concern about who has access to their data and whether NHS data will be shared with other Government departments (e.g. Home Office, DWP).
- Examples of poorly designed digital and AI technologies compounding worse health outcomes and inequalities for some groups – for example, pulse oximetry being less accurate for darker skinned people, contributing to health inequality.
- Some evidence of higher risks of exposure to online harms (online abuse, hate speech, harassment) with harmful effects on physical and mental health. This may have additional impacts on confidence, motivation and trust to use digital services.
- Lack of evidence found on specific digital access barriers. Some evidence of higher risks of exposure to online harms (online abuse, hate speech, harassment) with harmful effects on physical and mental health. This may impact on confidence, motivation and trust.
- Intersectionality with other protected characteristics and inclusion health groups; after accounting for ethnicity, some faith and belief groups are more likely to live in areas of deprivation (Muslim faith) or are at greater risk of poverty than other faiths (Sikh faith).
- Some Haredi Jewish communities rely on written/print media for communications.
- Differences between men and women’s access to and use of digital technology appear more impacted by other factors such as age, disability, living circumstances (e.g. if living alone or with someone else) than by sex.
- Women are more likely to be older and have a disability or long-term condition; women are also more likely to live alone in older age. All these correlate with lower internet access and use.
- Women and men are differently represented in inclusion health groups (e.g. most lone parents are women; most ex-offenders are men).
- Women face higher risks than men of exposure to online harms (online abuse, hate speech, harassment) with harmful effects on physical and mental health. This may impact on their confidence, motivation and trust to use digital services.
- Lack of evidence on specific digital access barriers. Some evidence of higher risks of exposure to online harms (online abuse, hate speech, harassment) experienced by LGBTQ+ groups, with harmful effects on physical and mental health. This may impact on confidence, motivation and trust.
4.2 Additional areas to consider for other groups at greater risk of health inequalities
This section picks up any specific or additional areas to consider for people in other groups or communities which may be more likely to experience barriers to accessing services and worse health outcomes – such as people in poverty or with low literacy. It also picks up additional areas to consider which have particular relevance to inclusion health groups – groups who face extreme social exclusion and the worst health outcomes. National data on internet access and use shows a strong correlation with low income and low educational attainment. National data on health inequalities shows strong correlations between these indicators, area deprivation and reduced health life expectancy.
Many of the insights about specific groups are drawn from qualitative research or the experience of voluntary and community sector organisations. While there is a clear high-level picture about digital exclusion as presenting additional risks to health inequalities, there is a need for more focused research – including on how digital inclusion (ensuring people have the access, skills and support; and making digital services inclusive by design) can improve access and health outcomes, and help to reduce health inequalities.
- Evidence of lower digital access and skills among children and young people in the looked after system and young care leavers
- Low skills, overlapping with low basic literacy and numeracy – impacts for digital, health and media literacy
- Housing circumstances, for example lack of WiFi, lack of private space
- Not being able to afford sufficient mobile data or suitable device
- Design of digital health or care services for young people may not reflect lower levels of literacy and digital literacy, or disability-related needs (higher in this group)
- Benefits to carers of accessing digital health and care services can be significant
- Supporting them in their caring roles (e.g. convenience, flexibility around work and other roles, saving time and money)
- Supporting greater independence, choice and control of those they care for
- Supporting wider quality of life for them and the person they care for
- Barriers to digital access and use intersect strongly with age and disability
- Most unpaid carers are older people caring for a spouse or partner (and may not see themselves as a carer)
- More older people care for an older parent and/or for grandchildren, including older parents of disabled adults, adults with learning disabilities
- Fewer older people are aware of or benefit from assistive technology and knowing how to adjust devices to make them more accessible
- Community-based services and support to help people use the internet can be harder for carers to access due to less time and caring responsibilities
- Living on a low or very low income, and ‘financial vulnerability’ are among the strongest predictors of digital exclusion across all ages (both non-use of the internet, and also using the internet but only for a very few things)
- Not being able to afford:
- A suitable device (intersects with disability where the cost of a suitable device and additional impairment-related kit can be higher)
- Sufficient data connectivity (intersects with disability, and poor literacy – where people may also need more time to access a digital service)
- Sufficient electricity to keep digital devices charged (this may be a more important factor in the months ahead with energy price rises)
- Some evidence that people in lower socio-economic status households are less likely to be active in encouraging other people they know to stay safe online
- Evidence shows strong correlation between local area deprivation and factors which correlate closely with digital exclusion including: low income, high unemployment, low educational attainment.
- Some deprived areas may experience worse signals and lower speed – which could relate to quality of mobile and broadband infrastructure, types of housing provision (including social and private rented provision) and population density
- Some areas of deprivation will have low levels of community infrastructure – e.g. lack of community services and support within walking distance, which is free to access and well resourced; other areas of deprivation may have strong community infrastructure and support networks.
- There’s some evidence that people in lower socio-economic status households are less likely to be active in encouraging other people they know to stay safe online.
- There is a strong correlation between low internet access and low or limited use of the internet and having low educational attainment, including low basic literacy
- Increased risk of low health literacy and low media literacy (e.g. not knowing where to find trustworthy health information or apps online)
- Additional barriers in finding and understanding health information online, and around tasks such as form filling (e.g. booking or confirming appointments)
- No or poor access due to no mobile or broadband coverage; weak signals and slow speed affect the quality of user experience even if there is internet access
People experiencing homelessness, rough sleeping or insecure housing
- Not having a suitable device and/or not being able to afford enough connectivity;
- Hostels vary in their provision of digital access and WiFi for service users
- Libraries, GPs, and other local settings vary in how trusted or welcoming they are, and their provision of digital access and WiFi for service users
- Lack of private space to enable confidential use of digital health services
- Smartphones are very useful for people on the street but extreme poverty and dealing with addictions or mental health problems makes it harder to hang onto a phone as an item of value and that requires charging and money for data.
- Lower digital skills compounded by lower / less regular internet access
- Trust and mistrust issues with technology (e.g. surveillance) and with digital public services (e.g. data being shared with other government departments)
- Barriers to accessing services linked to no fixed address / housing circumstances
- Identity verification barriers to registering for online NHS and GP services
- Low health literacy and understanding about how health and care systems work
- Differences in entitlements by citizenship status for some homeless people.
People involved in the criminal justice system (offenders in prison / on probation; ex-offenders)
- Restricted internet access for people in prison – impacting on confidence and skills to use the internet upon release from prison
- Not having a suitable device and/or not being able to afford enough connectivity
- Lower digital skills compounded by lower / less regular internet access
People with addictions and substance misuse problems
- Intersectionalities with other inclusion health groups – e.g. experience of addictions and substance misuse problems and/or homlessness or insecure housing and/or experience of the criminal justice system and/or experience of trauma
- Not having a suitable device and/or not able to afford enough connectivity
- Lower digital skills compounded by lower / less regular internet access
- Trust and mistrust issues with technology – and with digital public services
- Lack of private space to enable confidential use of digital health services
People in other inclusion health groups – including refugee and migrant communities, people seeking asylum; Gypsy, Roma and Traveller communities
- Not having a suitable device and/or not able to afford enough connectivity
- Lower digital skills compounded by lower / less regular internet access
- Trust and mistrust issues with technology (e.g. surveillance) and with digital public services (e.g. data being shared with other government departments)
- Lack of private space to enable confidential use of digital health services
- Identity verification barriers to registering for online NHS and GP services
- Low health literacy and understanding about how health and care systems work
- Differences in entitlements by citizenship status for some homeless people
Section 5: Useful research and resources
This section provides a list (not exhaustive) with hyperlinks to useful resources. The sections below cover: resources on digital exclusion and health inequalities (including NHS guidance); resources relevant to protected characteristics; resources relevant to other groups at greater risk of health inequalities.
This list of resources was not developed through a systematic review, and does not claim to be exhaustive or comprehensive. It was developed by Good Things Foundation – as part of Good Things Foundation’s role in the VCSE Health and Wellbeing Alliance (2021/2022).
If you are aware of a key resource or toolkit or evidence review which you feel should be included in a future iteration of this guide, please contact Good Things Foundation’s research team.
Contact details: research@goodthingsfoundation.org
NHS Guidance and resources
A Plan for Digital Health and Social Care – Department of Health and Social Care’s plan (2022)
Putting data, digital and tech at the heart of transforming the NHS – Independent report by Laura Wade-Gery (2021)
NHS Transformation Directorate: Involving people and communities in digital services – Guidance for health and social care digital teams on how to involve people in their work
NHS Digital Service Manual – A service manual for designers and developers of digital services
NHS Digital: Digital inclusion for health and social care (revised July 2019) – A guide to help healthcare providers, commissioners and designers
NHS: Accessible Information Standard and related public-facing resources (NHS & Sense 2017)
NHS Transformation Directorate: Digital Technology Assessment Criteria
NHS England: Working in partnership with people and communities (draft statutory guidance)
NHS Futures Collaboration Platform (registration required)
Other research and resources on digital and health inequalities
Ada Lovelace Institute, Tackling health and social inequalities in data-driven systems
Covid-19 Committee 2021, Beyond digital: planning for a hybrid world. House of Lords
Good Things Foundation 2021, Digital exclusion and health inequalities: A briefing
Good Things Foundation 2020, Digital inclusion in health and care: Lessons learned from the NHS Widening Digital Participation programme
Good Things Foundation 2020, Digital Health Hubs evaluation (WSA consultants)
Gov.uk Health Equity Assessment Tool (HEAT)
Health Education England, Digital literacy of the wider workforce toolkit
Health Foundation 2020, The Health Foundation Covid-19 Survey
Healthwatch England 2021, Locked out: Digitally excluded people’s experiences of remote GP appointments
Healthwatch England & National Voices 2020, The Doctor Will Zoom You Now
House of Commons 2020, Unequal impact? Coronavirus, disability and access to services
Inclusion Health 2020, Inclusion Health Audit Toolkit
Leeds Healthwatch 2020a, Digitizing Leeds: Risks and opportunities
Leeds Healthwatch 2020b, Digital inclusion in Leeds: How does it feel for me?
LGA 2020, Digital Innovation in Adult Social Care. Local Government Association
National Voices 2021, Unlocking the digital front door: keys to inclusive health care
Public Health Wales 2020, Digital technology and health inequalities: A scoping review
Thrive by Design 2022, Inclusive digital transformation in mental health: What you need to know
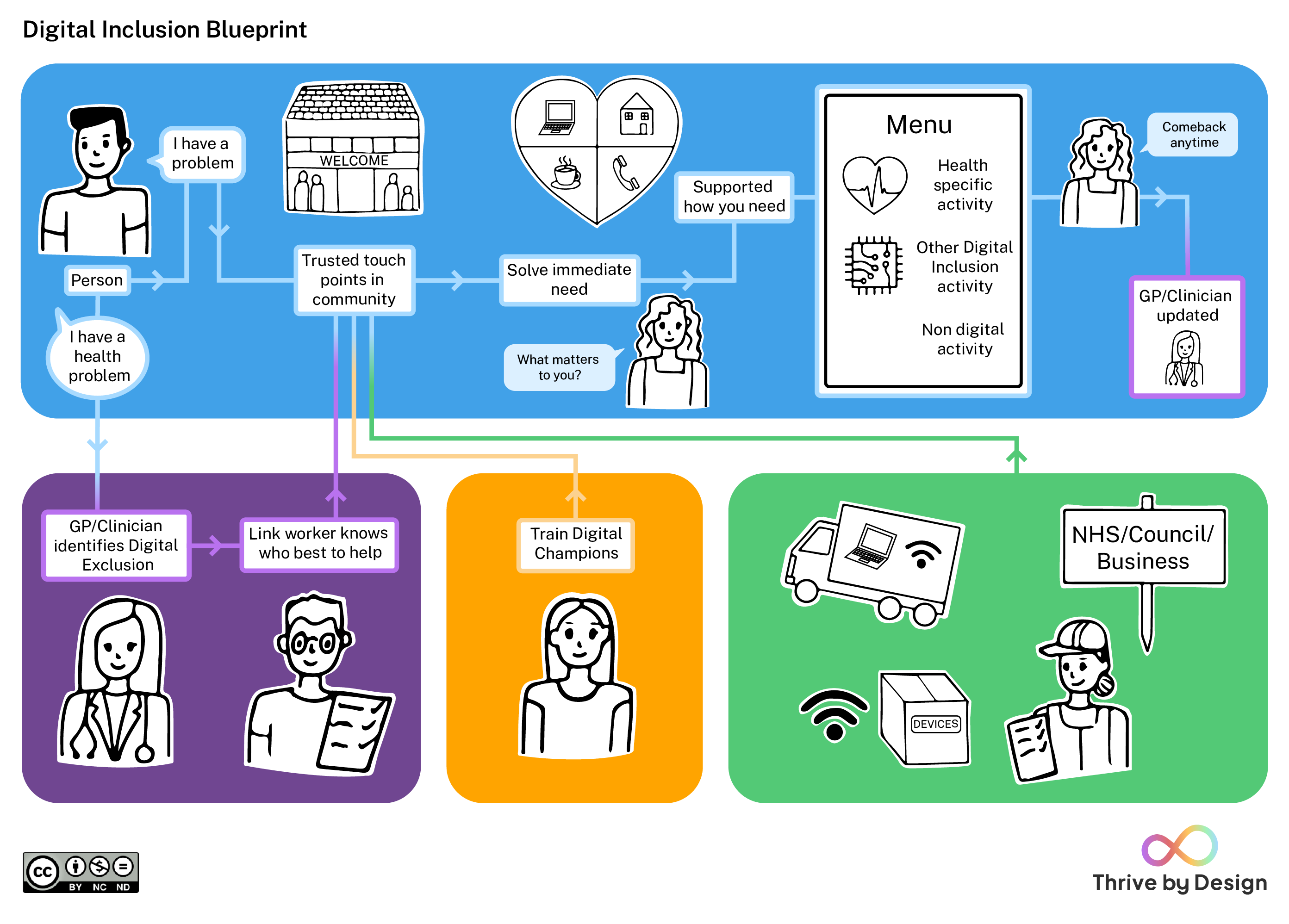
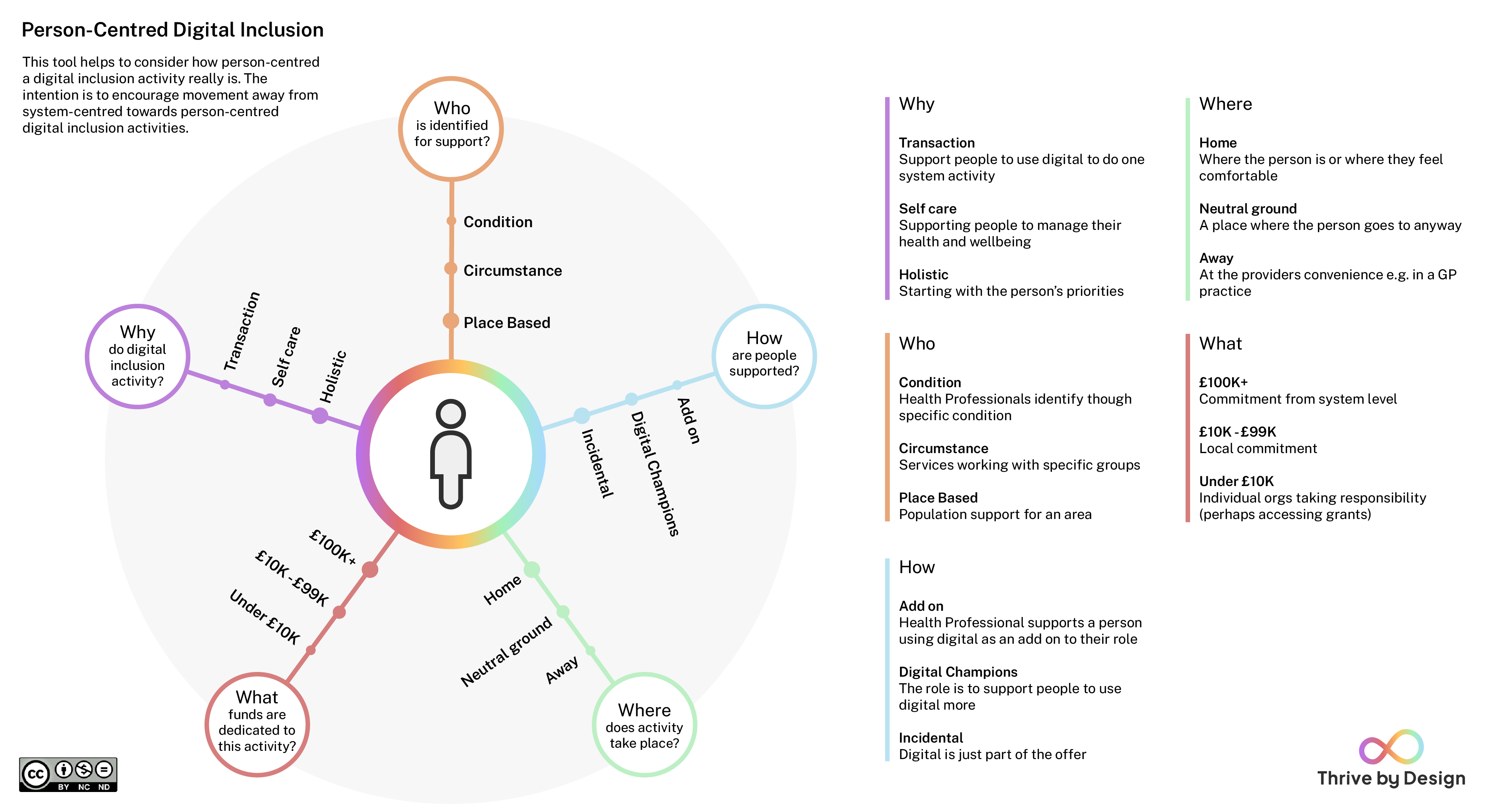
Thrive by Design 2022, Digital inclusion tools for integrated care systems (with Digital inclusion blueprint visual and Person-centred Digital inclusion visual)
{kind=link}
{kind=link}
Forthcoming: Basis Social with Good Things Foundation: barriers and enablers to uptake of digital services in health and social care for people with basic access and skills (for NHS England)
Resources on digital exclusion and inclusion (general, not specific to health)
Cebr 2022, The economic case for digital inclusion in the UK
Good Things Foundation 2022, Digital Nation 2022 (infographic with data sources)
Good Things Foundation 2021, Digital inclusion and online safety for adults in the UK
Ofcom 2022, Adults’ Media Use and Attitudes (series of reports updated annually)
Ofcom 2022, Affordability of communications services (series of research reports, updated)
ONS Centre for Equalities and Inclusion 2019, Exploring the UK’s digital divide (stand-alone)
Lloyds Banking Group 2021, UK Consumer Digital Index (series of reports, updated annually)
Lloyds Banking Group 2021, UK Essential Digital Skills Benchmark (third annual report)
Age
Age UK 2020, Not like riding a bike. Why some older people stop using the internet.
Age UK 2021, Digital inclusion and older people: how have things changed in a Covid-19 world? Briefing paper.
Age UK 2022, Age UK’s Digital Instruction Guides.
British Red Cross 2021, Life after lockdown: Tackling loneliness.
Carnegie UK Trust 2017, #NotWithoutMe: Digital exclusion among vulnerable young people.
Catch 22, 2021, Digital disadvantage: Barriers to digital skills and access (young people)
Good Things Foundation 2022, Doing digital in later life: A practical guide; Supporting evidence.
Good Things Foundation 2018, I am connected. New approaches to supporting people in later life. Centre for Ageing Better.
Housing LIN 2021, TAPPI Inquiry: Technology for an Ageing Population Panel for Innovation.
NIHR ARC Greater Manchester 2022, Older people’s access to digitalised services.
Nominet Digital Youth Index – annual report and benchmarking tool
Reengage 2022, Online in your 80s: Lifeline or waste of time?
Forthcoming from UKRI Healthy Ageing Challenge research and innovation, for example the Generating Older Active Lives Digitally project.
Disability and long-term conditions
AbilityNet resources – including guides on Website Accessible Guidelines
Digital Communities Wales 2021, Good practice guide to digital for care homes.
Good Things Foundation 2020, Dementia and digital participation for health and wellbeing.
Good Things Foundation 2022, Digital Lifeline Fund: A qualitative evaluation (evaluating a government funded programme to address digital exclusion of people with learning disabilities)
Housing LIN 2021, TAPPI Inquiry: Technology for an Ageing Population Panel for Innovation.
NHS Confederation 2020, Digital inclusion in mental health toolkit. With Association of Mental Health Providers.
NHSX 2021, Adult Social Care Technology and Digital Skills Review. With Ipsos Mori, Institute of Public Care, Skills for Care, and Local Government Association.
Ofcom 2018, Access and Inclusion report.
Seale 2020, Using technology to support people with learning disabilities stay connected during lockdown. Open University.
Skills for Care 2015, Common core principles to support self-care.
Thrive by Design 2022, Adopting inclusive digital transformation in mental health: Discovery findings report; a Thrive by Design project commissioned by NHS England.
Thrive by Design 2022, Inclusive digital transformation in mental health: Knowledge into action briefing.
Gender reassignment
Unaware of specific evidence on digital exclusion and health.
On online abuse: Evelyn, S et al 2022, ‘A Phenomenological Investigation into Cyberbullying as Experienced by People Identifying as Transgender or Gender Diverse’, International Journal of Environmental Research and Public Health 2022, 19(11).
Marriage and civil partnership
Unaware of specific evidence on digital exclusion and health
Pregnancy and maternity
Public Health England 2018, Bright Beginnings: support for vulnerable migrant and refugee women during the perinatal period
NHS Digital Maternity programme
NHS 2021, Equity and equality – Guidance for local maternity systems
Babies in Lockdown 2021, ‘No-one wants to see my baby’
Babies in Lockdown 2020, Listening to parents to build back better
Race and ethnicity
NHS Race and Health Observatory 2022, Ethnic inequalities in healthcare: A rapid evidence review. [Includes a section on Ethnic Inequalities in Digital Inclusion and Access to Health Services.]
NHS Race and Health Observatory 2021, Pulse oximetry and racial bias.
Doctors of the World 2020, A rapid needs assessment of excluded people in England during the 2020 Covid-19 pandemic
Friends, Families and Travellers 2018, Digital exclusion in Gypsy and Traveller communities in the United Kingdom.
Good Things Foundation 2020, Supporting digital inclusion of adults with low English language skills
On online abuse, for example: Glitch with End Violence Against Women (2020), The Ripple Effect: Covid 19 and the pandemic of online abuse.
Forthcoming publication insights report and standards on using Equality Impact Assessments for new treatments and disruptive innovations commissioned by the NHS Race and Health Observatory and produced by the Health Innovation Network.
Religion and belief
Unaware of specific evidence on digital exclusion and religion and belief
Sex
Largely addressed in relation to other protected characteristics or health inequalities
Sexual orientation
Unaware of specific evidence on digital exclusion and sexual orientation
On online abuse: Abreu R & Kenny M 2018, ‘Cyberbullying and LGBTQ Youth: A Systematic Literature Review and Recommendations for Prevention and Intervention’, Journal of Child & Adolescent Trauma 2018, 11(1).
Looked after and accommodated children and young people
Carnegie UK Trust 2017, #NotWithoutMe: Digital exclusion among vulnerable young people
Catch 22 2021, Digital disadvantage: Barriers to digital skills and access
Carers (unpaid family members)
Carers UK 2021, State of Caring 2021 Report
ParentZone 2021, Digital poverty: what still needs to happen
People on low incomes and/or living in areas of deprivation
Cambridge University and Newcastle University 2021, Levelling up health: A practical, evidence based framework (limited on digital exclusion)
Good Things Foundation 2022, Towards solving data poverty
Good Things Foundation 2021, Digital exclusion and health inequalities: a briefing
Health Foundation, Useful publications and resources on healthy lives for all
Institute for Health Equity 2020, The Marmot Review Ten Years On (limited on digital exclusion)
Joseph Rowntree Foundation 2014, Reducing poverty in the UK: Collection of evidence reviews
Joseph Rowntree Foundation 2021, UK Poverty 2020/21
Local Trust 2021, Making connections: Community-led action on data poverty
Ofcom 2022, Adults’ media use and attitudes report
Public Health Wales 2020, Digital technology and health inequalities: A scoping review
People who have low literacy
Good Things Foundation 2020, Digital inclusion in health and care: Lessons learned from NHS Widening Digital Participation (on health and digital literacy)
Patient Information Forum 2020, Health and Digital Literacy Survey 2019/20
Rowlands 2020, Health literacy and digital literacy (Newcastle University)
People living in remote, rural or island areas
Public Health Wales 2020, Digital technology and health inequalities: A scoping review
Across inclusion health groups
Inclusion Health 2020, Inclusion Health Audit Toolkit
Friends, Families & Travellers, Inclusion Health Self Assessment Tool for Primary Care Networks
Gov.UK, Inclusion Health: Applying All our Health
Thrive by Design 2022, Digital inclusion tools for integrated care systems
University of Cambridge, Inclusive Design Toolkit and Exclusion Calculator
People experiencing homelessness, rough sleeping and insecure housing
Homeless Link – Coproduction toolkit
Homeless Link – Reboot UK resources for digital skills
Homeless Link – Health Needs Audit tool
Good Things Foundation – Reboot UK: Final evaluation report
Pathway, Homeless Digital Template
Pathway 2017, Improving Digital Health Access for Excluded Groups
See ‘Digital health and people with complex lives’ in Good Things Foundation 2020
People involved in the criminal justice system
Unaware of specific resources – intersectionality with other inclusion health groups such as people experiencing homelessness and insecure housing.
People with addictions and substance misuse problems
Unaware of specific resources – intersectionality with other inclusion health groups such as people experiencing homelessness and insecure housing.
See also ‘Digital health and people with complex lives’ in Good Things Foundation 2020
People who are refugee, migrants or seeking asylum
Good Things Foundation 2020, Digital inclusion of adults with low English language skills
Research underway led by British Red Cross (a VCSE Health and Wellbeing Alliance project).
People in Gypsy, Roma and Traveller communities
About Good Things Foundation
Good Things Foundation is the UK’s leading digital inclusion charity. Between 2013-2016 and 2017-2020, Good Things Foundation partnered with NHS England and NHS Digital to deliver the ‘Widening Digital Participation’ programme. Good Things Foundation is the charity behind the National Databank, National Device Bank, and National Digital Inclusion Network (‘online centres’). For more information: Fix the Digital Divide – For Good: Strategy 2022-25
Good Things Foundation has undertaken this work in its role as a member of the VCSE Health and Wellbeing Alliance. The Voluntary Community and Social Enterprise (VCSE) Health and Wellbeing Alliance (HW Alliance) is a partnership between sector representatives and the health and care system. It enables the sector to share its expertise at a national level with the aim of improving services for all communities. The HW Alliance is jointly managed by the Department of Health and Social Care (DHSC), NHS England, UK Health Security Agency and Office for Health Improvement and Disparities and is made up of 18 VCSE Members that represent communities who share protected characteristics or that experience health inequalities and a VCSE coordinator.